

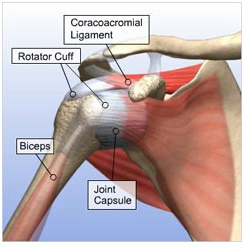
The rotator cuff is formed by the tendinous portions of four muscles – the supraspinatus, infraspinatus, teres minor and the subscapularis which arise from the scapula (shoulder blade) and attach to the upper end of the humerus (arm bone). The rotator cuff serves three important functions: 1. To move the arm in relation to the scapula 2. To stabilize the head of the humerus in the glenoid fossa socket 3. To achieve muscular balance (fine tuning) at the shoulder joint
This is also known as Shoulder impingement syndrome, Painful arc syndrome or Mid-arc syndrome. Shoulder impingement is described as pain or discomfort felt by a patient on forward flexion of the arm (lifting the arm in the front of the body). This literally means that the rotator cuff gets pinched between the acromion and the upper end of humerus. Typically the pain begins when the arm is raised to about 60 degrees and continues until the arm reaches about 120 degrees. As the arm is moved beyond this point the pain disappears. Similarly, when the patient tries to lower the arm from a fully elevated (flexed) position, the pain appears at about 120 degrees and disappears when it reaches about 60 degrees. This is described as ‘mid-arc syndrome’ as the pain appears in the middle range of full flexion of 180 degrees. The presence of impingement merely points to the involvement of the rotator cuff as the cause of patient’s shoulder pain. It may be caused either due to rotator cuff tendinitis or a partial tear or full thickness tear of the rotator cuff.
There are two types of Impingement of Shoulder Joint primary & secondary
Primary Impingement:
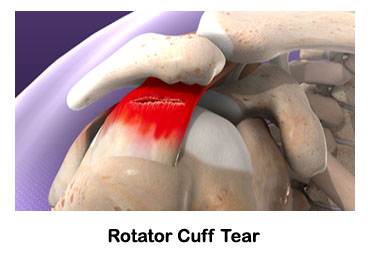
It is caused whenever there is tendinitis (swelling) or tear (partial or full thickness) of the rotator cuff. The causes are
This refers to weakening of the rotator cuff due to degeneration of ageing, which could lead to partial or full thickness tears and are seen in middle-aged and elderly patients.
This refers to tears caused due to a violent fall on the hand, and is seen in both young as well as old patients.
This is due to deposition of calcium crystals in the rotator cuff which may cause tendonitis (inflammation) or tear.
Inflammation of the subacromial bursa which lies under the acromion.
These are bony outgrowths arising from under surface of the acromion or from an arthritic acromio-clavicular (AC) joint. These spurs can rub against the rotator cuff causing impingement.
Secondary impingement:
Impingement can also be caused when the cuff is normal but gets impinged due to instability of the shoulder. This instability could be due to excessive stretching of the anterior capsule or the rotator cuff due to repetitive throwing motion as in throwing athletes.
Diagnosis of a patient with impingement is made on the basis of patient’s symptoms, physical examination and investigations like Ultrasonography and MRI scan. Patients with primary impingement present with pain on the outer aspect of the shoulder especially on forward flexion (elevation of the arm in the front of the body). On examination these patients will have a positive impingement test (Neer’s and Hawkin’s test). They usually have some limitation of internal rotation (difficulty in getting the hand behind the patient’s back). They may have weakness of strength of rotator cuff muscles. Patients with secondary impingement due to associated instability of the shoulder will demonstrate a positive Apprehension test and Jobe’s relocation test. Patients with long-standing full thickness tears develop severe arthritic changes in shoulder and have marked pain, stiffness and severe disability. This is known as rotator cuff arthropathy.
This is useful in imaging rotator cuff tears. Its accuracy for diagnosing full thickness tears is high.
MRI remains the best imaging modality for rotator cuff dysfunction. It is a very sensitive test with high accuracy rates. It can distinguish between tendinitis, intra-substance tears, partial tears and full thickness tears. The addition of contrast arthrography further increases its accuracy.
The treatment of impingement depends upon the cause of impingement (rotator cuff tendinitis or tear, subacromial bursitis, acromial spur or calcific tendonitis).Treatment modalities include rest, anti-inflammatory medication, physiotherapy and surgery. Most patients with tendinitis and partial tears will respond to non-operative treatment.
This is particularly useful in patients with acute and severe pain. Once pain subsides patients should be encouraged to use their arm. Athletes may need gradual resumption of training activities.
This includes modalities for relieving pain (heat treatment), stretching exercises (for stretching the tight posterior capsule), and exercises for strengthening the rotator cuff. Throwing athletes will need corrective measures to improve their throwing action.
This is reserved for patients who do not respond to the above treatment options. The surgical options include:
Acromioplasty (Subacromial decompression): This involves removing the bony spur or prominence on the under surface of the acromion. Acromioplasty alone suffices if there is no cuff tear. This can be done by arthoscopic surgery. Arthroscopic surgery has the advantage of being minimally invasive, and causes lesser trauma to the deltoid muscle, and therefore allows faster recovery.
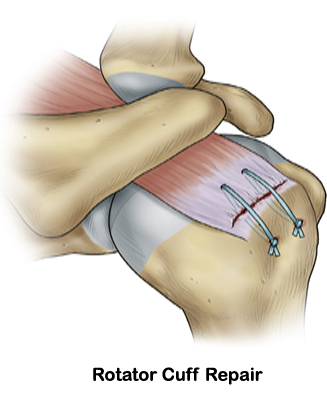
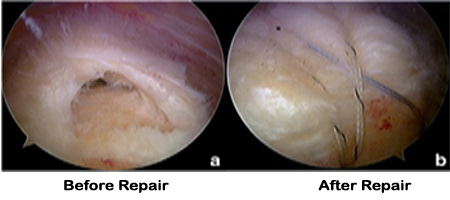
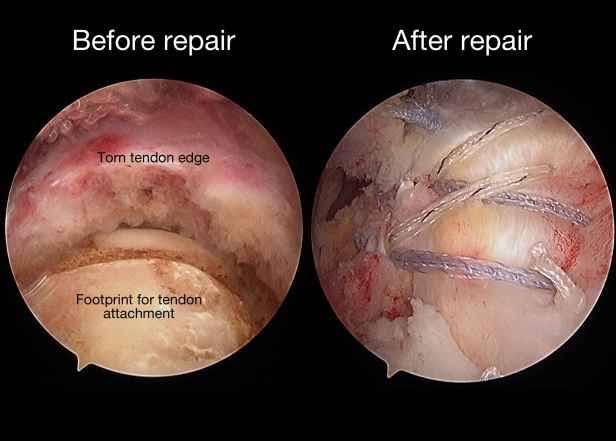
Rotator cuff repair: This involves repairing the torn rotator cuff back to the bone at its site of insertion on the humerus. Full thickness tears are re-attached back to bone using suture anchors. Partial thickness tears are usually treated with debridement (cleaning up of the torn surface) with a view to stimulate healing. Both these procedures may be done arthroscopically or by open surgery.
Reverse shoulder replacement: This is usually required in patients with rotator cuff arthropathy (severe arthritis due to long standing massive rotator cuff tear) with severe disability. The reverse shoulder arthroplasty has been shown to give good results in these patients.
Website Designed By: Quick n Host
